
Yesterday I felt privileged to have been invited to a discussion in Parliament promoted by the All-Party Parliamentary Group for Prescribed Drug Dependence, in partnership with the Council for Evidence-based Psychiatry.
The objective of the meeting was to discuss evidence of the link between the rise in disability claimants and the record level of antidepressant prescribing. The UK Department of Health has recently released data which shows that over 61 million prescriptions for antidepressants (costing £285 million) were issued in England alone in 2015, a rise of 7% on the previous year and over double the figure in 2005.
 Host Paul Flynn MP (left) began the event by introducing the main speaker, the Pulitzer-shortlisted science journalist and author Robert Whitaker, who said: “There is substantial evidence in the scientific literature that antidepressants increase the chronicity of the disorders they are used to treat, and increase the risk that a person will become disabled. The data, I believe, lead to a very disturbing conclusion: the dramatic rise in disability for depression and anxiety seen across the western world is being caused, in large part, by the very drugs which are being used to treat them.”
Host Paul Flynn MP (left) began the event by introducing the main speaker, the Pulitzer-shortlisted science journalist and author Robert Whitaker, who said: “There is substantial evidence in the scientific literature that antidepressants increase the chronicity of the disorders they are used to treat, and increase the risk that a person will become disabled. The data, I believe, lead to a very disturbing conclusion: the dramatic rise in disability for depression and anxiety seen across the western world is being caused, in large part, by the very drugs which are being used to treat them.”
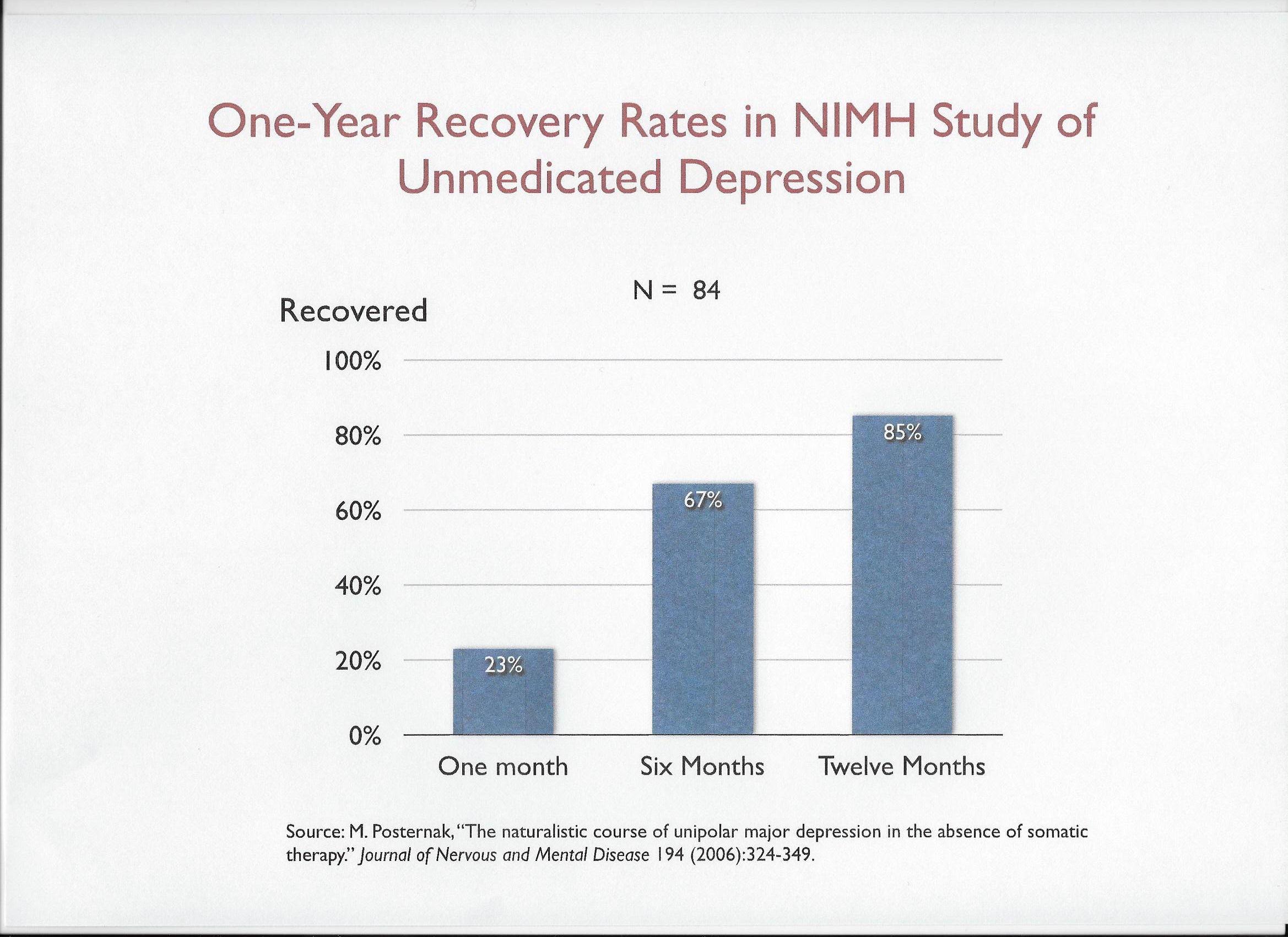
 In the space of a little over the half-hour that he was allotted, Robert (right) produced an astonishing array of evidence and data from several countries which showed how long-term use of antidepressants could lead to worse outcomes for patients. In quick succession he displayed a total of 51 slides, showing that, for example, patients are more likely to recover from an episode of depression if they remain unmedicated:
In the space of a little over the half-hour that he was allotted, Robert (right) produced an astonishing array of evidence and data from several countries which showed how long-term use of antidepressants could lead to worse outcomes for patients. In quick succession he displayed a total of 51 slides, showing that, for example, patients are more likely to recover from an episode of depression if they remain unmedicated:
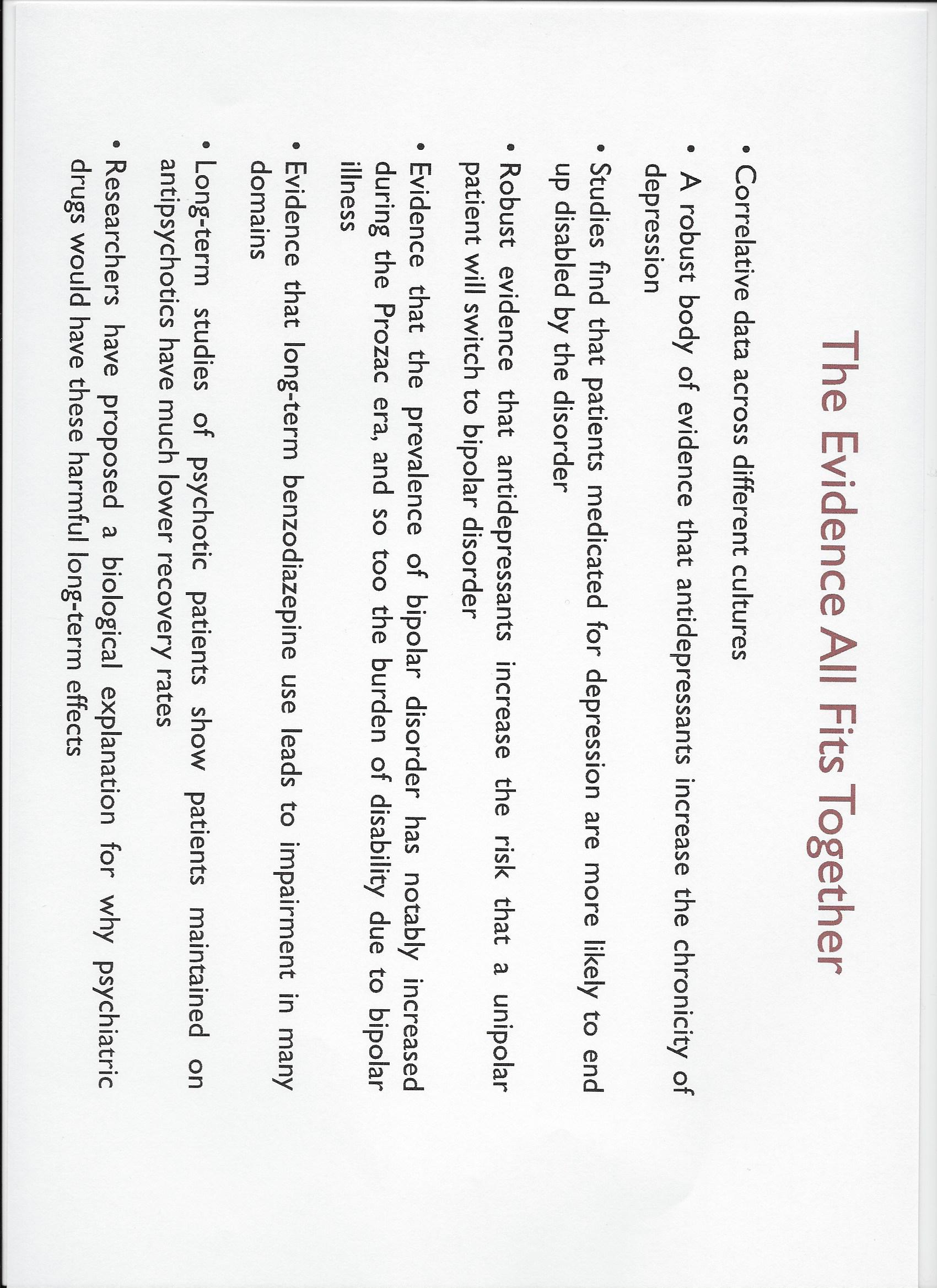
He also had data to show that patients on long-term prescriptions for other mind-altering medication, such as benzos or anti-psychotics, could face similar outcomes to those on antidepressants.
Robert’s final slide summed up the evidence that he had presented:
 After Robert’s speech, moderator Peter Kinderman introduced the members of the panel in turn. The first to speak was Paul Brett (left), who described how a virus led to a prescription for Prozac (Fluoxetine) and other antidepressants. He spent several years in horrific withdrawal from the drugs, leading to the loss of his flourishing career and the disruption of almost every other aspect of his life.
After Robert’s speech, moderator Peter Kinderman introduced the members of the panel in turn. The first to speak was Paul Brett (left), who described how a virus led to a prescription for Prozac (Fluoxetine) and other antidepressants. He spent several years in horrific withdrawal from the drugs, leading to the loss of his flourishing career and the disruption of almost every other aspect of his life.
 The next speaker was Allan Young (right) from King’s College, London, whose rôle on the panel was to rebut Robert Whitaker’s argument. Allan began by comparing antidepressants to penicillin in that they were beneficial, but not suited to everybody, and churlishly dismissed Robert’s arguments and evidence as “soundbites”. He was no more convincing than he was when arguing against Peter Gøtzsche at last May’s More Harm than Good debate. Allan, incidentally, has received payment from several pharmaceutical companies, including Lundbeck, makers of Citalopram, and Eli Lilly (Fluoxetine).
The next speaker was Allan Young (right) from King’s College, London, whose rôle on the panel was to rebut Robert Whitaker’s argument. Allan began by comparing antidepressants to penicillin in that they were beneficial, but not suited to everybody, and churlishly dismissed Robert’s arguments and evidence as “soundbites”. He was no more convincing than he was when arguing against Peter Gøtzsche at last May’s More Harm than Good debate. Allan, incidentally, has received payment from several pharmaceutical companies, including Lundbeck, makers of Citalopram, and Eli Lilly (Fluoxetine).
 Allan was followed by Sami Timimi (left), a consultant psychiatrist who specialises in the mental health of children. Sami was obviously worried about the damage that antidepressants can do to children, and placed emphasis on a “therapeutic alliance” founded on more effective training and commissioning, as well as wider public education about emotional health.
Allan was followed by Sami Timimi (left), a consultant psychiatrist who specialises in the mental health of children. Sami was obviously worried about the damage that antidepressants can do to children, and placed emphasis on a “therapeutic alliance” founded on more effective training and commissioning, as well as wider public education about emotional health.
 Following Sami was Joanna Moncrieff (right) from University College London, who has recently completed research on disability benefits. This shows that the number of claimants for mental disorders rose by 103% from 1995 to 1.1 million in 2014, while claimants for other conditions fell by 35% in the same period. Two thirds of mental disorder claimants in 2014 were classified as having a depressive or anxiety disorder. Her research showed that: “It may well be that, for various reasons, the drugs are in fact contributing to the disability burden, resulting in significant social and economic costs.”
Following Sami was Joanna Moncrieff (right) from University College London, who has recently completed research on disability benefits. This shows that the number of claimants for mental disorders rose by 103% from 1995 to 1.1 million in 2014, while claimants for other conditions fell by 35% in the same period. Two thirds of mental disorder claimants in 2014 were classified as having a depressive or anxiety disorder. Her research showed that: “It may well be that, for various reasons, the drugs are in fact contributing to the disability burden, resulting in significant social and economic costs.”
Joanna explained that a “chemical imbalance” does not exist, and never did. There has been no effective study as to what SSRIs can do to people, and no evidence that they work. There is also evidence to show that they can harm unborn babies. She said that antidepressants are “disempowering”, as long-term use presents the dilemma of problems when withdrawal is attempted, as well as reducing motivation in the individual’s approach to life.
Joanna was followed by a GP, Andrew Green (left) of the BMA. Andrew outlined the difficulties faced by the prescriber who would like to reduce prescribing, but who has limited time and resources to assist those who are troubled by what life has sent their way.
 The final member of the panel to speak was Philippa Stroud (right) of the Centre for Social Justice. She spoke with feeling about the link she has witnessed between social deprivation and overuse of antidepressants, often prescribed against NICE guidelines. She saw short patient contact time linked with poor prescribing practices, and insufficient encouragement of non-medicinal interventions. Of particular distress to her was the medicating of childhood, and lives damaged from difficulties in the earliest years by children unable to voice their problems or escape them. Philippa called this the “Silent Scream”.
The final member of the panel to speak was Philippa Stroud (right) of the Centre for Social Justice. She spoke with feeling about the link she has witnessed between social deprivation and overuse of antidepressants, often prescribed against NICE guidelines. She saw short patient contact time linked with poor prescribing practices, and insufficient encouragement of non-medicinal interventions. Of particular distress to her was the medicating of childhood, and lives damaged from difficulties in the earliest years by children unable to voice their problems or escape them. Philippa called this the “Silent Scream”.
 Peter Kinderman then called for comments or questions from the audience. Among the contributors were two activists whom I have come to know personally, Millie Kieve (left), founder of APRIL, and Katinka Newman, who spoke eloquently about her ordeal on antidepressants. Katinka, incidentally, has recently completed a book about her experiences.
Peter Kinderman then called for comments or questions from the audience. Among the contributors were two activists whom I have come to know personally, Millie Kieve (left), founder of APRIL, and Katinka Newman, who spoke eloquently about her ordeal on antidepressants. Katinka, incidentally, has recently completed a book about her experiences.
The final contributors from the audience were two experts for whom I have great respect, John Read and James Davies, both of whom have been mentioned previously in this website.
Others attending the event included clinical psychologist Lucy Johnstone, professor of psychiatry Sheila Hollins, founder member of the CEP Luke Montagu, and the Shadow Minister for Mental Health Luciana Berger.
 In his closing summary, Peter Kinderman (right) called for future action both in terms of undertaking more research and addressing current prescribing practices. He reminded the audience that there was a political angle to the over-prescription of antidepressants, and that the problem could not be addressed properly until social equality improved.
In his closing summary, Peter Kinderman (right) called for future action both in terms of undertaking more research and addressing current prescribing practices. He reminded the audience that there was a political angle to the over-prescription of antidepressants, and that the problem could not be addressed properly until social equality improved.
Paul Flynn closed the event, with the express wish that progress be achieved.
Update: a complete video recording of the event is now available for viewing on YouTube.

More reviews of the meeting:
Can Psychiatry At Least Be Curious? by Robert Whitaker
Report from the latest meeting of the APPG for Prescribed Drug Dependence by James Davies
High antidepressant use could lead to UK public health disaster by Clare Wilson
Related Articles:
Antidepressants and the Politics of Health
The Council for Evidence-based Psychiatry
How Antidepressants Ruined Luke’s Life
Our son went to the GP and he said to him, “So you are feeling a bit down? Lacking enthusiasm? Okay, well try this antidepressant [Citalopram]. It is a mild little drug – I have over 200 patients on it.”
Our son took it and was psychotic by 2am. We contacted the doctor, and he said, “Keep taking it for at least another week.”
However, after a third night of screaming and thinking the TV could hear him, we stopped and that was the start of our son’s mental health issues. The more drugs they kept giving him, the worse he got. Olanzapine, Quetiapine, Risperidone, Lithium, Depakote, with each effort more and more problems. He would be convinced people were after him and that the BBC was broadcasting his thoughts.
Anyway, we stopped the drugs and the psychotic symptoms have disappeared after about 6 months. A wise man told me that depression should be construed as deep rest and doing nothing is good for you.
GPs in particular mistake sadness for clinical depression. Dr Sarah Jarvis said the other night that moderate and severe depression kills people. It does not, it is the mind-altering drugs that make people take their lives – I have never seen an inquest where the suicide victim was not on medication.
My son Josh, aged 23, was under the local Crisis Team for two years with a night psychotic condition and, for about the last 8 months of his life, was in supported accommodation, with only day support.
He was on Olanzapine and, reflecting back, it would seem that his loss of being able to think and function for everyday tasks, due to medication, made his 16 hrs work a week impossible and added to his problems and anxiety.
Despite Josh being classed as severely disabled (and claiming sick we found out afterward), his benefit and housing benefit (we discovered afterwards) had been suspended, which must have added to his anxiety in the last week of his life.
British Transport Police visited us on the 31st December 2013 to say he had been killed on the railway. The train driver’s statement indicated it was a deliberate act.
I recall being prescribed and taking Dothiepin, then Moclobemide, for years, myself, but neither helped. After many EEG tests and brain scans, it was discovered I had atrophy of the brain, which I feel is responsible for my non-epileptic episodes and health issues.