This is the fourth in the annual series of Lost Children posts, in which I recall the children who lost their lives after being prescribed antidepressants, and whose inquests have been reported during the past year.
I also include links to other inquests where there was no specific report in the media of antidepressants being prescribed, although it seemed likely that psychiatric medication may well have had some involvement. What all these inquests had in common, however, is that in each case the child had been receiving treatment from medical professionals at or before the time of his or her death.
The National Institute for Health and Care Excellence (NICE) recognises that antidepressants can induce suicidal ideation in patients of all ages. This is why, in NICE Clinical Guideline 90 (Depression in adults), it recommends that antidepressants should be only used for “moderate to severe depression”. For “sub-threshold” symptoms such as anxiety or grief, “the risk-benefit ratio is poor”.
 When it comes to prescribing antidepressants to children under 18, the guidelines are unequivocal. In NICE Clinical Guideline 28 (Depression in children and young people), NICE effectively regards them as a “last resort” option. It stipulates three criteria, all of which must be met if antidepressants are to be prescribed.
When it comes to prescribing antidepressants to children under 18, the guidelines are unequivocal. In NICE Clinical Guideline 28 (Depression in children and young people), NICE effectively regards them as a “last resort” option. It stipulates three criteria, all of which must be met if antidepressants are to be prescribed.
Two of these are straightforward:
- Only if the child has been diagnosed with moderate to severe clinical depression.
- Only if it can be shown that the prescription has been preceded by an extended period of “specific interpersonal therapy” which has proved ineffective.
The third, however, is somewhat contentious: practitioners are not supposed to prescribe any of the available SSRIs (eg Citalopram, Sertraline or Seroxat) with the irrational exception of Fluoxetine (aka Prozac). This decision goes back to evidence supplied by manufacturers Eli Lilly, which was later exposed as fraudulent.
There is no valid, independent evidence to show that Eli Lilly’s Fluoxetine is any “safer” for children than other SSRIs. If NICE would accept that the dangers of prescribing Fluoxetine were the same as prescribing all other SSRIs, then there would be no good reason to prescribe antidepressants to children. But suggestions to NICE are merely forwarded to the MHRA, a regulatory body totally funded by Pharma, and staffed in some of its more important positions by ex-Pharma employees.
It can be seen from the summaries below that, in every single case, at least one of the criteria laid down by NICE had been completely ignored by practitioners who were supposed to be looking after the children. It is especially disturbing that many of the children were treated not only by their own GP, but by the local Child and Adolescent Mental Health Services (CAMHS). Those who work for CAMHS are deemed to be specialists in the area of children’s mental health. Yet, time after time, they are either unaware of the NICE Guidelines, or they choose to ignore them.
This number of children mentioned this year is significantly smaller than in the previous years. I would like to be able to say that this is due to the number of children taking their lives had declined, when it is probable that the opposite is true.
A smaller proportion of self-inflicted deaths are now reported in the media, particularly where children are concerned. Of those that are reported, coverage is, on the whole, perfunctory. Often, basic details appear in print after a death, but the inquest itself is not reported in the local or national newspapers.
Reputable organisations such as the Samaritans have asked for limited reporting of self-inflicted deaths, believing that: “Inappropriate reporting of suicide may lead to ‘imitative’ behaviour…For example, if young people are provided with details about the method of suicide used, it can lead to more deaths using the same method.”
 The most widely-read article on my site during the past year followed the inquest of 16-year-old schoolgirl Rachel Finke from North London, which was not reported at all in the media. Rachel’s mother Sarah contacted me, and allowed me to publish her heart-rending account of the final year of the life of her energetic, talented daughter, who was never diagnosed with depression. In January 2016, Rachel was referred to CAMHS by her GP after scratching her arms. Without instigating any form of therapy, Rachel was prescribed Fluoxetine. She reacted badly to this and, 3 weeks later, she attempted suicide. The Fluoxetine was withdrawn immediately and replaced a few days later by Melatonin and Mirtazapine. In the next two months, Rachel overdosed twice and the Mirtazapine was withdrawn. She continued to take Melatonin for the rest of her life, even though it comes with a heightened suicide risk, “especially for people who are female, 10-19 old, have been taking the drug for 1-6 months.” There were more overdoses and self harming, and in December she was prescribed Sertraline. Five weeks later, and 8 days after the dosage was doubled, Rachel walked out of school and took her life.
The most widely-read article on my site during the past year followed the inquest of 16-year-old schoolgirl Rachel Finke from North London, which was not reported at all in the media. Rachel’s mother Sarah contacted me, and allowed me to publish her heart-rending account of the final year of the life of her energetic, talented daughter, who was never diagnosed with depression. In January 2016, Rachel was referred to CAMHS by her GP after scratching her arms. Without instigating any form of therapy, Rachel was prescribed Fluoxetine. She reacted badly to this and, 3 weeks later, she attempted suicide. The Fluoxetine was withdrawn immediately and replaced a few days later by Melatonin and Mirtazapine. In the next two months, Rachel overdosed twice and the Mirtazapine was withdrawn. She continued to take Melatonin for the rest of her life, even though it comes with a heightened suicide risk, “especially for people who are female, 10-19 old, have been taking the drug for 1-6 months.” There were more overdoses and self harming, and in December she was prescribed Sertraline. Five weeks later, and 8 days after the dosage was doubled, Rachel walked out of school and took her life.
 Last year I listed the inquest of Heather Blower from Manchester, who was 18 when she took her life. This year, Heather’s mother Paula, a healthcare assistant, wrote to me and told me the shocking events that preceded Heather’s death. Heather suffered from social anxiety and found her job an ordeal. Her GP signed her off work and referred her to CAMHS where, while Heather was still 17, a psychiatrist told Paula that Heather was depressed, and would be prescribed Fluoxetine. About four weeks later, Heather cut her wrist badly enough to be taken to A&E. Paula suspected an adverse reaction to Fluoxetine, but was told by the psychiatrist that Heather should continue to take it. After a few weeks, Paula decided to taper the dosage, and two months later Heather was free of medication and her mood had improved. In the meantime, her social anxiety had not been addressed, her sick note had expired and she was no longer being paid sickness benefit. Heather went to see a GP, who said he would sign a note only if Heather agreed to accept a prescription of Fluoxetine. Heather told her mother that she would not take the pills, but started to take them secretly. Two days after Christmas, Heather was found by her twin sister Heidi, hanged in her bedroom.
Last year I listed the inquest of Heather Blower from Manchester, who was 18 when she took her life. This year, Heather’s mother Paula, a healthcare assistant, wrote to me and told me the shocking events that preceded Heather’s death. Heather suffered from social anxiety and found her job an ordeal. Her GP signed her off work and referred her to CAMHS where, while Heather was still 17, a psychiatrist told Paula that Heather was depressed, and would be prescribed Fluoxetine. About four weeks later, Heather cut her wrist badly enough to be taken to A&E. Paula suspected an adverse reaction to Fluoxetine, but was told by the psychiatrist that Heather should continue to take it. After a few weeks, Paula decided to taper the dosage, and two months later Heather was free of medication and her mood had improved. In the meantime, her social anxiety had not been addressed, her sick note had expired and she was no longer being paid sickness benefit. Heather went to see a GP, who said he would sign a note only if Heather agreed to accept a prescription of Fluoxetine. Heather told her mother that she would not take the pills, but started to take them secretly. Two days after Christmas, Heather was found by her twin sister Heidi, hanged in her bedroom.
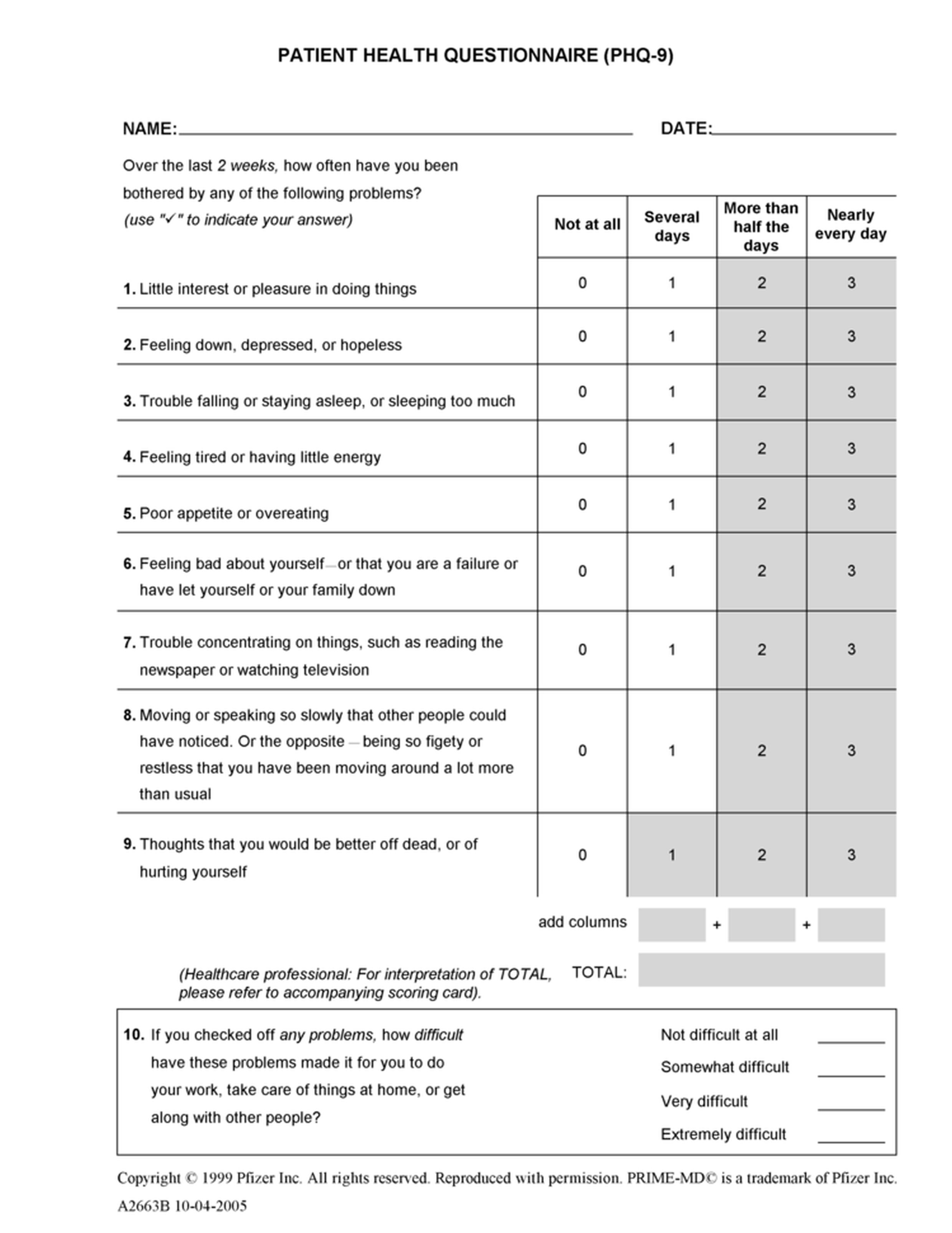
One of the many shocking aspects of Heather’s treatment was that the diagnosis of depression that she received at CAMHS emanated from a computer. In all likelihood, this was the PHQ-9 Patient Health Questionnaire, a facile 9-question multiple-choice quiz that cannot differentiate between clinical depression and short-term anxiety. This fraudulent program was promoted by the pharmaceutical company Pfizer, who originally owned the intellectual property and distribution rights. Pfizer also manufacture Venlafaxine and Sertraline, two of the most commonly prescribed antidepressants in the UK.
 (click to enlarge)
(click to enlarge)
 Of those whose inquest details I reported myself, the youngest victim was Sophie Clark, a 13-year-old schoolgirl from Dorset who was a talented writer and artist. Sophie had lost her mother at the age of 3, and was brought up by her father. After a diagnosis of depression, she was prescribed antidepressants and received counselling. At her inquest in January, a psychiatrist and the deputy head teacher at her school both said that her mood was improving when, one evening in June 2016, Sophie told her father that she was going for a walk. The next morning, a dog-walker found her hanging in nearby woodland. The coroner said: “I think there was nothing that could have been done that could have prevented this.”
Of those whose inquest details I reported myself, the youngest victim was Sophie Clark, a 13-year-old schoolgirl from Dorset who was a talented writer and artist. Sophie had lost her mother at the age of 3, and was brought up by her father. After a diagnosis of depression, she was prescribed antidepressants and received counselling. At her inquest in January, a psychiatrist and the deputy head teacher at her school both said that her mood was improving when, one evening in June 2016, Sophie told her father that she was going for a walk. The next morning, a dog-walker found her hanging in nearby woodland. The coroner said: “I think there was nothing that could have been done that could have prevented this.”
 Stephen Mortimer was a 14-year-old schoolboy from Lancashire. He excelled at computer studies, but had been diagnosed with autism, and struggled to cope with anxiety. In the summer term of 2016, Stephen had problems with some fellow-pupils and the head teacher suggested that his GP should refer him to CAMHS. At the end of the term, Stephen moved to a new school, where he was noticeably happier. However, at his inquest in July, a psychiatrist at CAMHS said that he decided to prescribe him Sertraline which would reduce his agitation. In fact, as the following term approached, Stephen became more agitated and, the day before term was due to begin in January, he hanged himself in the back garden.
Stephen Mortimer was a 14-year-old schoolboy from Lancashire. He excelled at computer studies, but had been diagnosed with autism, and struggled to cope with anxiety. In the summer term of 2016, Stephen had problems with some fellow-pupils and the head teacher suggested that his GP should refer him to CAMHS. At the end of the term, Stephen moved to a new school, where he was noticeably happier. However, at his inquest in July, a psychiatrist at CAMHS said that he decided to prescribe him Sertraline which would reduce his agitation. In fact, as the following term approached, Stephen became more agitated and, the day before term was due to begin in January, he hanged himself in the back garden.
 15-year-old Josie James from North Wales was described by her mother at her inquest in March as “a fun-loving and quirky young woman who loved people”. When she was 13, Josie told her parents that she was hearing voices in her head and, in January 2014, Josie was referred to CAMHS. After a year of treatment by CAMHS, which included changes of medication, Josie’s mental health had deteriorated to such an extent that in January 2015 she was prescribed anti-psychotic drugs. Following the prescription, Josie’s mental health continued to decline and, in May 2015, she was admitted to a mental health unit. Two months later, Josie decided to stop taking the medication that she had been prescribed. Even so, she was discharged from the unit after she was declared “not suicidal nor at risk of self-harm”. In August 2015, after visiting a friend in hospital at Bangor, Josie jumped from the Menai Bridge. The coroner delivered a narrative verdict, criticising the ineffective communication with Josie’s family, in matters such as her assessment, her diagnosis, the changes in her medication and the fact that she had stopped taking medication.
15-year-old Josie James from North Wales was described by her mother at her inquest in March as “a fun-loving and quirky young woman who loved people”. When she was 13, Josie told her parents that she was hearing voices in her head and, in January 2014, Josie was referred to CAMHS. After a year of treatment by CAMHS, which included changes of medication, Josie’s mental health had deteriorated to such an extent that in January 2015 she was prescribed anti-psychotic drugs. Following the prescription, Josie’s mental health continued to decline and, in May 2015, she was admitted to a mental health unit. Two months later, Josie decided to stop taking the medication that she had been prescribed. Even so, she was discharged from the unit after she was declared “not suicidal nor at risk of self-harm”. In August 2015, after visiting a friend in hospital at Bangor, Josie jumped from the Menai Bridge. The coroner delivered a narrative verdict, criticising the ineffective communication with Josie’s family, in matters such as her assessment, her diagnosis, the changes in her medication and the fact that she had stopped taking medication.
 Last year, I wrote an article after the death of Brandon Singh Rayat, a 15-year-old schoolboy from Leicester. He had become so upset by bullying that he refused to go to school. After a visit from an attendance officer, Brandon was referred to CAMHS and was prescribed Fluoxetine. His mother Mina said: “He was on antidepressants, but the dose got higher, and each time it did, he seemed to get worse in himself. He told the psychiatrist he had flashbacks of hanging himself.” An inquest in August this year heard that Brandon had attempted to take his life shortly after being prescribed Fluoxetine. In August last year, after about 7 months on ever-higher doses of the drug, Brandon hanged himself at home. Mina has launched an anti-bullying campaign in memory of Brandon, and is striving to make bullying a criminal offence.
Last year, I wrote an article after the death of Brandon Singh Rayat, a 15-year-old schoolboy from Leicester. He had become so upset by bullying that he refused to go to school. After a visit from an attendance officer, Brandon was referred to CAMHS and was prescribed Fluoxetine. His mother Mina said: “He was on antidepressants, but the dose got higher, and each time it did, he seemed to get worse in himself. He told the psychiatrist he had flashbacks of hanging himself.” An inquest in August this year heard that Brandon had attempted to take his life shortly after being prescribed Fluoxetine. In August last year, after about 7 months on ever-higher doses of the drug, Brandon hanged himself at home. Mina has launched an anti-bullying campaign in memory of Brandon, and is striving to make bullying a criminal offence.
 In December 2016, 15-year-old Pippa McManus stepped in front of a train at Gatley Station in Manchester. When she was 12, she had started to be obsessive about her weight, and was referred to CAMHS. The following year, Pippa was detained under the Mental Health Act and admitted to the Priory in Altrincham. At her inquest in May, Pippa’s father Jim described some of the care she received as “disturbing”. A Serious Case Review, published in October, showed that he was justified in making that remark. It revealed that: “On 5th March 2015…Pip’s mood appeared low and agitated. Pip’s consultant recommended Pip commence on Fluoxetine to treat low mood, agitation and obsessive compulsive thoughts…the dose was started on 10mg and later increased to 20mgs per day on 13th March 2015.” The following month, Pip began to voice thoughts of suicide: “Pip, who was already on a prescription of Fluoxetine, opposed the consultant’s plan to increase the level to help manage the high level of obsessive compulsive symptoms…An urgent treatment order was authorised to prescribe the higher dose without Pip’s consent.” Pippa was also prescribed Promethazine (a sedative) and Olanzapine (anti-psychotic).
In December 2016, 15-year-old Pippa McManus stepped in front of a train at Gatley Station in Manchester. When she was 12, she had started to be obsessive about her weight, and was referred to CAMHS. The following year, Pippa was detained under the Mental Health Act and admitted to the Priory in Altrincham. At her inquest in May, Pippa’s father Jim described some of the care she received as “disturbing”. A Serious Case Review, published in October, showed that he was justified in making that remark. It revealed that: “On 5th March 2015…Pip’s mood appeared low and agitated. Pip’s consultant recommended Pip commence on Fluoxetine to treat low mood, agitation and obsessive compulsive thoughts…the dose was started on 10mg and later increased to 20mgs per day on 13th March 2015.” The following month, Pip began to voice thoughts of suicide: “Pip, who was already on a prescription of Fluoxetine, opposed the consultant’s plan to increase the level to help manage the high level of obsessive compulsive symptoms…An urgent treatment order was authorised to prescribe the higher dose without Pip’s consent.” Pippa was also prescribed Promethazine (a sedative) and Olanzapine (anti-psychotic).
 Just hours after leaving a psychiatric unit in February 2016, 15-year-old schoolgirl Rosemary Pedley hanged herself in her bedroom at her home in a Staffordshire village. At her inquest in March, the coroner was told that Rosemary had a history of depression and self-harm and “had been on the sort of antidepressants usually prescribed for adults.” A consultant at the unit said that they had tried a number of treatments to help Rosemary, including drugs and therapy. He added: “She seemed to be improving and said she felt a lot better.”
Just hours after leaving a psychiatric unit in February 2016, 15-year-old schoolgirl Rosemary Pedley hanged herself in her bedroom at her home in a Staffordshire village. At her inquest in March, the coroner was told that Rosemary had a history of depression and self-harm and “had been on the sort of antidepressants usually prescribed for adults.” A consultant at the unit said that they had tried a number of treatments to help Rosemary, including drugs and therapy. He added: “She seemed to be improving and said she felt a lot better.”
 15-year-old Becky Romero had been treated by CAMHS in Bristol for several years when, in June, she took an overdose of medication. There was no room available for her at the local adolescent residential unit, and she was sent to the nearest available unit, 125 km away in Bournemouth. In December, Becky’s inquest heard that, before she was discharged 4 weeks later, she was prescribed “new medication”. The medication was, in fact, Fluoxetine, and Becky told her parents that she was feeling side effects. On July 19th, Becky was found hanged in her bedroom. The coroner expressed concerns around the support in place for Becky, given that she had just been prescribed a new drug, Fluoxetine, which “could cause increased agitation and increased risk of self-harm”. She also pointed out that guidelines state that when Fluoxetine is prescribed to young people, they should be carefully monitored for side effects but, days after it was given to Becky, she was sent home and did not see a mental health professional face-to-face again before her death.
15-year-old Becky Romero had been treated by CAMHS in Bristol for several years when, in June, she took an overdose of medication. There was no room available for her at the local adolescent residential unit, and she was sent to the nearest available unit, 125 km away in Bournemouth. In December, Becky’s inquest heard that, before she was discharged 4 weeks later, she was prescribed “new medication”. The medication was, in fact, Fluoxetine, and Becky told her parents that she was feeling side effects. On July 19th, Becky was found hanged in her bedroom. The coroner expressed concerns around the support in place for Becky, given that she had just been prescribed a new drug, Fluoxetine, which “could cause increased agitation and increased risk of self-harm”. She also pointed out that guidelines state that when Fluoxetine is prescribed to young people, they should be carefully monitored for side effects but, days after it was given to Becky, she was sent home and did not see a mental health professional face-to-face again before her death.
 One evening in December 2016, 16-year-old schoolboy Joe Pickhaver, described as “kind, with a quirky sense of humour”, was struck by a train on the line near his home in Whitstable. He had spent time in a mental health unit, from where a doctor told his inquest in March that he thought Joe had been feeling “hopeless and felt that no one could help him” but that he “felt safe at home“. He also told the court: “Even though Joe had been a low risk of suicide, he could have made a plan and not given it away to anyone. Joe was very intelligent and he could beat the system and he would know how to avoid detection.” He added: “He stopped his medication against his parents’ and my advice.” Joe actually resumed his medication a week before he died, but the court was told, wrongly, that “they usually take a few weeks to take effect.”
One evening in December 2016, 16-year-old schoolboy Joe Pickhaver, described as “kind, with a quirky sense of humour”, was struck by a train on the line near his home in Whitstable. He had spent time in a mental health unit, from where a doctor told his inquest in March that he thought Joe had been feeling “hopeless and felt that no one could help him” but that he “felt safe at home“. He also told the court: “Even though Joe had been a low risk of suicide, he could have made a plan and not given it away to anyone. Joe was very intelligent and he could beat the system and he would know how to avoid detection.” He added: “He stopped his medication against his parents’ and my advice.” Joe actually resumed his medication a week before he died, but the court was told, wrongly, that “they usually take a few weeks to take effect.”
 Talented photographer Ela Ozbayraktar was a 16-year-old schoolgirl from Oxfordshire. In November 2016, Ela was found hanging in her bedroom. Her inquest in March heard that Ela began therapy 8 months before her death, and “after being prescribed Fluoxetine she said her mood started to improve over the summer.” However, when she went back to school in September, Ela told one therapist that she started to go downhill again. Ela’s mother Magda said that the family “received all the support they could hope for from the school and mental health services.”
Talented photographer Ela Ozbayraktar was a 16-year-old schoolgirl from Oxfordshire. In November 2016, Ela was found hanging in her bedroom. Her inquest in March heard that Ela began therapy 8 months before her death, and “after being prescribed Fluoxetine she said her mood started to improve over the summer.” However, when she went back to school in September, Ela told one therapist that she started to go downhill again. Ela’s mother Magda said that the family “received all the support they could hope for from the school and mental health services.”
 On the morning of March 30th, 17-year-old Chloe Hillier, who was mother to a young son, was found hanged in a Blackpool park. At her inquest in September, her mother Louise described her as “a shy girl and an amazing mum”, but said that, due to problems with her boyfriend, she had been struggling in the months after the birth of her son. She went to see her GP, who prescribed Citalopram. Chloe had been staying in a mother and baby unit but had also been staying at her mother’s. On March 29th she told staff at the unit that she wanted to stay at her mum’s another night, but was told that she had to go back. Her mother told the inquest that she left the house at around 3pm.Some time later, she was captured on CCTV buying a rope at a garage.
On the morning of March 30th, 17-year-old Chloe Hillier, who was mother to a young son, was found hanged in a Blackpool park. At her inquest in September, her mother Louise described her as “a shy girl and an amazing mum”, but said that, due to problems with her boyfriend, she had been struggling in the months after the birth of her son. She went to see her GP, who prescribed Citalopram. Chloe had been staying in a mother and baby unit but had also been staying at her mother’s. On March 29th she told staff at the unit that she wanted to stay at her mum’s another night, but was told that she had to go back. Her mother told the inquest that she left the house at around 3pm.Some time later, she was captured on CCTV buying a rope at a garage.
An inquest in September heard that a gifted 17-year-old boy from Essex was found hanged at his home. He had been taking prescribed antidepressants, and was withdrawing from them at the time of his death.
Other teenagers whose inquests in 2017 revealed that they had lost their lives after taking antidepressants included: Ava Broom, Courtney Davis, George Cheese, Joel Ingram, Nathan Carmon and Sean Russell (all 18), and Ashleigh Martin, Jack Bucktrout, Kieran Duru, Michelle Mosot, Miranda Williams, Rowan Sollit and Sam Symons (all 19).
In the reports of inquests summarised below, there were no reports in the media that antidepressants had been prescribed. In each case, however, the child had been receiving some form of treatment from medical professionals at or before the time of his or her death. In the majority of instances, at least part of the child’s treatment was delivered by the local CAMHS.
 A week after his 13th birthday in August, Brandon Barker hanged himself at the bottom of the garden of his Colchester home. After the inquest in October, Brendan’s father Carl said that Brandon had been referred to a specialist for mental health problems and that a referral came through a month before he took his own life. He said that he had tried for two years to get something in place for him. “He had depression and anxiety, but one of the agencies dropped him…Brandon has been let down massively.”
A week after his 13th birthday in August, Brandon Barker hanged himself at the bottom of the garden of his Colchester home. After the inquest in October, Brendan’s father Carl said that Brandon had been referred to a specialist for mental health problems and that a referral came through a month before he took his own life. He said that he had tried for two years to get something in place for him. “He had depression and anxiety, but one of the agencies dropped him…Brandon has been let down massively.”
 In August, the inquest of 14-year-old Charlotte Baron from Rochdale took place. In September 2015, Charlotte was hospitalised after taking an overdose of paracetamol. Following the incident, social services and mental health workers were assigned to her. A psychiatric nurse who met with Charlotte on a number of occasions described her as a bright pupil who enjoyed school, loved her family had lots of good friends, but agreed with the coroner that she was “very low in mood and unhappy.” In February, Charlotte was found hanged in her bedroom wardrobe.
In August, the inquest of 14-year-old Charlotte Baron from Rochdale took place. In September 2015, Charlotte was hospitalised after taking an overdose of paracetamol. Following the incident, social services and mental health workers were assigned to her. A psychiatric nurse who met with Charlotte on a number of occasions described her as a bright pupil who enjoyed school, loved her family had lots of good friends, but agreed with the coroner that she was “very low in mood and unhappy.” In February, Charlotte was found hanged in her bedroom wardrobe.
 14-year-old Sofia Legg was found hanged at her home in Somerset in September 2016. In July, her inquest heard that her mother Sandy had taken Sofia to her GP in March 2015 after becoming worried about her low mood and teachers reporting signs of self-harm. The doctor referred her to CAMHS, but they decided that she did not meet the criteria for specialist support. In June 2016, Sofia’s GP made an “urgent referral” to CAMHS after the teenager said that she had been having suicidal thoughts. She was seen twice in July by a care co-ordinator who told Sandy that there was a six-month waiting list for cognitive behaviour therapy. The day before Sofia’s death, the care co-ordinator met with Sofia, who told her that she had put an item that could have been used for self-harm under her bed. Sandy told the inquest that the care co-ordinator “gave us a crisis plan, which included things like talking…No follow up appointment was made during this meeting but (the care co-ordinator) said she would speak to a psychiatrist and review the case to see whether medication was a good option and that she would contact me as soon as she had an answer.” Whether the care co-ordinator meant by this statement that she was thinking about commencing, stopping or changing Sofia’s medication was not reported. In November, the coroner’s PFD Report was published. Here, various appointments that Sofia had with her GP and CAMHS between April 2015 and September 2016 were summarised, but the coroner decided to make no mention of medication in his report.
14-year-old Sofia Legg was found hanged at her home in Somerset in September 2016. In July, her inquest heard that her mother Sandy had taken Sofia to her GP in March 2015 after becoming worried about her low mood and teachers reporting signs of self-harm. The doctor referred her to CAMHS, but they decided that she did not meet the criteria for specialist support. In June 2016, Sofia’s GP made an “urgent referral” to CAMHS after the teenager said that she had been having suicidal thoughts. She was seen twice in July by a care co-ordinator who told Sandy that there was a six-month waiting list for cognitive behaviour therapy. The day before Sofia’s death, the care co-ordinator met with Sofia, who told her that she had put an item that could have been used for self-harm under her bed. Sandy told the inquest that the care co-ordinator “gave us a crisis plan, which included things like talking…No follow up appointment was made during this meeting but (the care co-ordinator) said she would speak to a psychiatrist and review the case to see whether medication was a good option and that she would contact me as soon as she had an answer.” Whether the care co-ordinator meant by this statement that she was thinking about commencing, stopping or changing Sofia’s medication was not reported. In November, the coroner’s PFD Report was published. Here, various appointments that Sofia had with her GP and CAMHS between April 2015 and September 2016 were summarised, but the coroner decided to make no mention of medication in his report.
After the inquest of Annabel Lewis (15) in March, the Staffordshire coroner submitted a PFD report. He said that Annabel “had been anxious and suffering from low self-esteem for some time….She had been referred to CAMHS in November 2015 by her GP but that referral was not accepted.” She was referred again in October 2016 by her school, but she declined the appointment “because of difficulty accessing the venue.” On November 4th, after a phone conversation with her boyfriend, Annabel died by asphyxiation in her bedroom.
 Early in the morning of June 12th 2016,15-year-old Ceri Sheehan from Hertfordshire was found by his father hanged in the garden. His inquest in April heard that Ceri was known to be a talented photographer and maintained his own website. The inquest was also told that Ceri had been suffering from depression and had attempted suicide with an overdose of pills a year earlier. He was in regular contact with a psychiatrist who had diagnosed him with depression, ADHD, and Asperger’s Syndrome.
Early in the morning of June 12th 2016,15-year-old Ceri Sheehan from Hertfordshire was found by his father hanged in the garden. His inquest in April heard that Ceri was known to be a talented photographer and maintained his own website. The inquest was also told that Ceri had been suffering from depression and had attempted suicide with an overdose of pills a year earlier. He was in regular contact with a psychiatrist who had diagnosed him with depression, ADHD, and Asperger’s Syndrome.
On October 9th 2016, 15-year-old Joshua Jones was found hanged at home in Flintshire. His inquest in March was told that he had “a history of depression and self-harm” and that from April 2016 he had been under the care of CAMHS. The representative from CAMHS said that, although Joshua was troubled, there was no sign of a mental health disorder. She added that it came down to social pressures and impulsive behaviour. Joshua’s mother told how she tried to get him to engage with CAMHS, but felt her son would not say what troubled him, rather “what they wanted to hear”.
 After witnessing the violent death of a close friend in Bournemouth in July 2016, Ciara Witt (16) took an overdose of pills the following month, telling her mother that she “wanted to be with her friend.” Her inquest in October heard that she had been suffering from low mood, and was already in the care of CAMHS. In November 2016, not long after her friend’s funeral, Ciara was found hanged in the garage at her home.
After witnessing the violent death of a close friend in Bournemouth in July 2016, Ciara Witt (16) took an overdose of pills the following month, telling her mother that she “wanted to be with her friend.” Her inquest in October heard that she had been suffering from low mood, and was already in the care of CAMHS. In November 2016, not long after her friend’s funeral, Ciara was found hanged in the garage at her home.
 On June 11th this year, 16-year-old schoolgirl Jordan Keates was discovered hanged in the hallway of her foster family’s home in Kent. At her inquest in September, a statement from a nurse at CAMHS who saw Jordan four days before her death was read out by the coroner. It said that in February she had taken an overdose, but “in March and April she was still improving, she was more positive…and she wanted to go to college to pursue art.” Jordan’s foster-mother Louise, with whom she had been for the past year, said: “She was a very funny girl. She was brilliant at her art and had a great future ahead of her. She was the first child we have ever fostered. Her death just came out of nowhere. We do feel let down by mental health services. We weren’t made aware of how many times she had been seen by mental health carers.”
On June 11th this year, 16-year-old schoolgirl Jordan Keates was discovered hanged in the hallway of her foster family’s home in Kent. At her inquest in September, a statement from a nurse at CAMHS who saw Jordan four days before her death was read out by the coroner. It said that in February she had taken an overdose, but “in March and April she was still improving, she was more positive…and she wanted to go to college to pursue art.” Jordan’s foster-mother Louise, with whom she had been for the past year, said: “She was a very funny girl. She was brilliant at her art and had a great future ahead of her. She was the first child we have ever fostered. Her death just came out of nowhere. We do feel let down by mental health services. We weren’t made aware of how many times she had been seen by mental health carers.”

16-year-old Leah Hook hanged herself at home in Gloucestershire in April. An inquest in September heard that she had been stressed because of her mock GCSE exams, and had not gone to school that week. In June 2015, Leah’s mother, had been concerned about her after some self-harming and took her to see her GP. Following the appointment, she was referred to a support group but never followed up on it.
 The inquest of 16-year-old Daisy French from Sheffield took place in November. When she was 13, Daisy was diagnosed with Asperger’s and depression. After a period of treatment, she was referred to CAMHS after she told a doctor that she had started to hear voices and self-harm. In June 2016, she was given a diagnosis of “non-organic psychosis”, and Daisy wrote in her journal that she was “worried about what was going to happen” to her as she was moved into adult social care. Daisy’s mother told the inquest that her daughter was a “bright girl” and, in spite of her problems, had gone on to do very well at her GCSEs. In November 2016, Daisy was found in a distressed state at Meadowhall Station, and told a police officer how she had tried to take her own life on 10 occasions in that year alone. After she had been seen by doctors at hospital, Daisy was discharged. The same police officer spoke with Daisy after she was reported at Sheffield Station in March, where she had to be physically restrained to prevent her taking her life. This time, Daisy told the officer that she had tried to kill herself on 20 separate occasions. Again, Daisy was taken to hospital but discharged without being admitted. A month later, Daisy was struck and killed by a train at Meadowhall Station.
The inquest of 16-year-old Daisy French from Sheffield took place in November. When she was 13, Daisy was diagnosed with Asperger’s and depression. After a period of treatment, she was referred to CAMHS after she told a doctor that she had started to hear voices and self-harm. In June 2016, she was given a diagnosis of “non-organic psychosis”, and Daisy wrote in her journal that she was “worried about what was going to happen” to her as she was moved into adult social care. Daisy’s mother told the inquest that her daughter was a “bright girl” and, in spite of her problems, had gone on to do very well at her GCSEs. In November 2016, Daisy was found in a distressed state at Meadowhall Station, and told a police officer how she had tried to take her own life on 10 occasions in that year alone. After she had been seen by doctors at hospital, Daisy was discharged. The same police officer spoke with Daisy after she was reported at Sheffield Station in March, where she had to be physically restrained to prevent her taking her life. This time, Daisy told the officer that she had tried to kill herself on 20 separate occasions. Again, Daisy was taken to hospital but discharged without being admitted. A month later, Daisy was struck and killed by a train at Meadowhall Station.
 On January 24th, a concerned member of the public rang police after seeing a boy sitting on a grassy area near a flyover by Brighton Marina. Reuben Downes (17) told police officers he was fine and was just meditating, but police officers took him back to his house. He was assessed by a doctor who judged him to be suffering from a psychotic episode, and prescribed him medication. The previous year, Reuben had been referred to the mental health trust after suffering from anxiety, but his mental health had deteriorated after the death of his grandmother. Later that day, Reuben told his parents he was hearing voices in his head telling him to kill himself. But his mother told the inquest in July: “He reassured us he wasn’t going to listen to the voices.” Early the following morning, Reuben’s body was discovered beneath the flyover.
On January 24th, a concerned member of the public rang police after seeing a boy sitting on a grassy area near a flyover by Brighton Marina. Reuben Downes (17) told police officers he was fine and was just meditating, but police officers took him back to his house. He was assessed by a doctor who judged him to be suffering from a psychotic episode, and prescribed him medication. The previous year, Reuben had been referred to the mental health trust after suffering from anxiety, but his mental health had deteriorated after the death of his grandmother. Later that day, Reuben told his parents he was hearing voices in his head telling him to kill himself. But his mother told the inquest in July: “He reassured us he wasn’t going to listen to the voices.” Early the following morning, Reuben’s body was discovered beneath the flyover.
 17-year-old Elliot Hobson was living in supported accommodation in Manchester when he took his life in February 2013. His inquest in May was told that Elliot was a gifted and talented boy but had shown signs of behavioural problems from a young age. When he was 13 he received a referral for specialist mental health support. At the time of his death he was suffering with depression and had made previous attempts on his life. He was in the care of CAMHS, where the psychiatrist assigned to Elliot said that he had recently been diagnosed with Asperger’s.
17-year-old Elliot Hobson was living in supported accommodation in Manchester when he took his life in February 2013. His inquest in May was told that Elliot was a gifted and talented boy but had shown signs of behavioural problems from a young age. When he was 13 he received a referral for specialist mental health support. At the time of his death he was suffering with depression and had made previous attempts on his life. He was in the care of CAMHS, where the psychiatrist assigned to Elliot said that he had recently been diagnosed with Asperger’s.
 17-year-old Steffan Bonnot was living in a care home for “emotionally damaged children” when he died on New Year’s Day 2016. A two-part inquest heard that he had gone on an outing with staff and other children from the home. While the group stopped off at MacDonalds, Steffan made his way to Arundel Station, where he was struck by a train. A psychotherapist at home described him as “a damaged, vulnerable and disturbed boy”. A 44-page Serious Case Review made no mention of any medication which had been prescribed to him.
17-year-old Steffan Bonnot was living in a care home for “emotionally damaged children” when he died on New Year’s Day 2016. A two-part inquest heard that he had gone on an outing with staff and other children from the home. While the group stopped off at MacDonalds, Steffan made his way to Arundel Station, where he was struck by a train. A psychotherapist at home described him as “a damaged, vulnerable and disturbed boy”. A 44-page Serious Case Review made no mention of any medication which had been prescribed to him.
Anthony Rose (17) from Devon was found hanged at home in August 2016. His inquest in March heard that, in the past, Anthony had been known to misuse alcohol and illicit drugs, although none were found in his system at the time of his death. Anthony had been referred to CAMHS, but had stopped using the service in the month before his death and had reported that he was feeling more positive.
 One morning last July, 17-year-old Solly Betts was found hanged at home in Devon. He was planning on joining the army and had been studying at a nearby military academy. At his inquest in May, Solly’s instructor described him as: “A good student, one of our leaders,” but added that Solly was ‘too hard on himself’.” Solly had been to his GP to get “help”. He was then referred to CAMHS, but two clinicians deemed that his was a routine case and he died before he got an appointment.
One morning last July, 17-year-old Solly Betts was found hanged at home in Devon. He was planning on joining the army and had been studying at a nearby military academy. At his inquest in May, Solly’s instructor described him as: “A good student, one of our leaders,” but added that Solly was ‘too hard on himself’.” Solly had been to his GP to get “help”. He was then referred to CAMHS, but two clinicians deemed that his was a routine case and he died before he got an appointment.
As most suicides by children are not reported in the media, the summaries above refer to the inquests of a small minority of the children who have taken their lives in England or Wales. Reading through the reports of the avoidable deaths of these children, there has been in each instance an intervention by at least one medical professional. Yet, if psychiatric medication is mentioned at all at an inquest, it is usually at the instigation of a bereaved relative.
One has to ask why coroners and other experienced professionals who should be familiar with NICE Guidelines seem content to see them flouted, often to the ultimate cost of the children to whom medication is mis-prescribed.
During 2017, inquests reported in the media also included those of: Louie Fenton (12), Tyrese Glasgow (12), Arin Lyth (13), Beth Fitton (13), Chloe Morris (13), Gavin Mason (13) Megan Hoyle (14), Nyah James (14), Sam Abel (14), Daniel Long (15), Georgia Brown (15), Haris Chohan (15), Dagmara Przybysz (16), Jason Monks (16), Lee Ridgway (16), Mason Mercer (16), Rebecca de Roeper (16), Caitlain Wright (17), Charles Evenden (17), Joseph Beresford-King (17), Nicole Lever (17), Paige Carr (17), Saffron Pickering (17) and Scott Flavill (17)
Inquests that were opened in 2017 but not reported as having been completed include those of: Natasha Newell (14), Seb Morris (14), Ellie Long (15), Thomas Rowe (15), Amelia Willis (16), Georgia Walsh (16), Holly Broadhead (16), James Doherty (16), James Thwaites (16), Jasmine Bush (16), Dom Sowa (17), Matthew Jones (17) and Mia Titheridge (17).
Top image: Train Tracks by Bob Dylan
Related Articles:
The Lost Children (2014, 2015, 2016 & 2018)
Why we shouldn’t give Prozac to children
Were these children given Prozac?
Dana’s Human Rights – and ours
Jake, Aged 14 (Part One, Part Two & Part Three)
Outstanding work in highlighting the deaths that Pharma, regulators and suicide organisations are failing to.
Your tenacity is admirable. I know, from personal experience, how dark this subject is and how frustrating it can be fighting the system.
I salute you, sir.
Well done, Brian. Once again you are all our voices fighting for truth, for change.
Sadly we can’t do anything to bring our children back, but we can do everything to stop this happening to others.
This should be out there, on the news, in papers.
We should all join forces so we are heard. We should shout and not be silenced. We should form an army of grieving families world wide.
It’s time for change. Stop killing our loved ones with your poisonous, mind-altering drugs.
We know the truth, we will not be silenced, we’re not going away.