
In March 2014, 13-year-old Sophie Parkinson (top) was found hanged at her home in Liff, near Dundee, in Scotland.
 In December 2019, Sophie’s mother Ruth (left) told a journalist that Sophie “was a kind child who was quick to rush to help any person or animal in distress. She would have made a great nurse.”
In December 2019, Sophie’s mother Ruth (left) told a journalist that Sophie “was a kind child who was quick to rush to help any person or animal in distress. She would have made a great nurse.”
Ruth, who herself is a nurse, said that Sophie’s “sweet, sensitive nature” meant that she struggled when her parents’ marriage broke down, and she began suffering mental health problems from the age of nine.
Ruth also said that she believed that her daughter would still be alive if she had received better care, and that previous suicide attempts were dismissed by medics as “childish cries for help”. She continued: “I believe that there were huge system failures in Sophie’s care. One time I called CAMHS (Child and Adolescent Mental Health Services) and there was no out of hours response available. People do not always have a crisis during office hours.
“Time after time, Sophie was not believed, and my pleas were ignored. I think because Sophie came from a good family and had a good home, her mental health problems were not taken as seriously. There were good times when Sophie could appear so bubbly and happy, but that’s not a reflection of someone’s true mental state. I wasn’t believed when I knew something was really wrong.”
On Monday August 10th this year, more than six years after her death, the Fatal Accident Inquiry finally began online, with the sheriff, procurator fiscal, lawyers and witnesses all appearing remotely. Ruth told the inquiry: “It’s true to say in the last few months of her life Sophie was exceptionally difficult to manage. She wasn’t getting any better. I wanted her to get better.”
 On the second day of the inquiry, therapist Stephen Thomson (right) said that Sophie had been referred to CAMHS by a self-harm team, and that “Sophie was a young person who came to the service and we wanted her to have the best care she possibly could.” He added that he felt that there had been a “good package of care” and that handling such cases could often be a “challenge” and a “tricky balance“.
On the second day of the inquiry, therapist Stephen Thomson (right) said that Sophie had been referred to CAMHS by a self-harm team, and that “Sophie was a young person who came to the service and we wanted her to have the best care she possibly could.” He added that he felt that there had been a “good package of care” and that handling such cases could often be a “challenge” and a “tricky balance“.
Evidence was presented by Dr Caroline Smith of CAMHS on the third day. She admitted that she did not complete a formal written assessment, but said she was continually assessing the teenager through a number of ongoing individual therapy sessions.
On the fourth day of the inquiry, Ruth said that she felt that she did not receive enough information about Sophie’s medication. She also criticised the fact she was never given a formal diagnosis of her daughter’s mental health issues, despite her being prescribed antidepressants.
 Dr Luke McQuitty (left) admitted that there was no formal diagnosis carried out on Sophie and that she was being treated for symptoms related to several issues. These included what he described as “depressive episodes” along with several other factors including attachment issues, anxiety, problems with interpersonal relationships, self-harm and suicidal ideation. He also said that he was continually assessing Sophie’s risk of self-harm during every appointment.
Dr Luke McQuitty (left) admitted that there was no formal diagnosis carried out on Sophie and that she was being treated for symptoms related to several issues. These included what he described as “depressive episodes” along with several other factors including attachment issues, anxiety, problems with interpersonal relationships, self-harm and suicidal ideation. He also said that he was continually assessing Sophie’s risk of self-harm during every appointment.
 On the fifth day, the inquiry heard from three expert witnesses. Consultant psychologist Dr John Marshall (right) said that the risk assessment by CAMHS was flawed, as it “relied too heavily on what Sophie was telling clinicians, rather than taking into account what the school or what her mother was telling them.”
On the fifth day, the inquiry heard from three expert witnesses. Consultant psychologist Dr John Marshall (right) said that the risk assessment by CAMHS was flawed, as it “relied too heavily on what Sophie was telling clinicians, rather than taking into account what the school or what her mother was telling them.”
 Dr Mischa Mockett (left), who specialises in child and adolescent psychiatry, told the court: “There is that slight possibility her death could have been avoided if absolutely everything was in place but it’s never that easy. It can’t be predicted. People are always going to complete suicide and we can’t protect against that.”
Dr Mischa Mockett (left), who specialises in child and adolescent psychiatry, told the court: “There is that slight possibility her death could have been avoided if absolutely everything was in place but it’s never that easy. It can’t be predicted. People are always going to complete suicide and we can’t protect against that.”
 Dr Aileen Blower (right),vice-chair of the child and adolescent faculty in Scotland for the Royal College of Psychiatrists, said that she believed that the service should have elevated Sophie to a “high-risk” category when her mental health rapidly worsened. She added: “The actual severity of the self-harm was not high, the pervasive suicidal thinking was of real concern…The family were asking for respite – that’s a big ask for a family that is very self-sufficient. Something was seriously wrong but the problem is we don’t know what.”
Dr Aileen Blower (right),vice-chair of the child and adolescent faculty in Scotland for the Royal College of Psychiatrists, said that she believed that the service should have elevated Sophie to a “high-risk” category when her mental health rapidly worsened. She added: “The actual severity of the self-harm was not high, the pervasive suicidal thinking was of real concern…The family were asking for respite – that’s a big ask for a family that is very self-sufficient. Something was seriously wrong but the problem is we don’t know what.”
After a gap of six days, the sixth and final day of the inquiry took place yesterday. Advocates continued to discuss the lack of a formal risk assessment as well as a lack of communication from CAMHS.
 Sheriff Lorna Drummond (left) concluded the procedure by stating that everything in a “complex picture” would be considered before she makes her final judgment.
Sheriff Lorna Drummond (left) concluded the procedure by stating that everything in a “complex picture” would be considered before she makes her final judgment.
Throughout the six days of the inquiry, daily summaries of the evidence and information from the various protagonists were provided by two Dundee-based newspapers, the Courier and the Evening Telegraph.
During this period, the only reference to Sophie’s medication regime recorded in the press came from her mother who, on the fourth day, said that she was not given enough information about Sophie’s medication, and that she was never given a formal diagnosis, “despite her being prescribed antidepressants”.
I did not read any information in the press about which drug(s) Sophie was prescribed, whether the dosage or the brand was altered, whether other psychotropic drugs were added or withdrawn, or whether the antidepressants were taken regularly. All of these factors would have had a bearing on Sophie’s state of mind, particularly in the last few months of her life.
 Last October, an article in the Herald revealed that the number of children aged 10 to 14 who were taking antidepressants had increased by 280% during the last decade. John Read (right), a professor of clinical psychology, described this figure as “alarming”. He added: “We just have no idea what effect these chemicals have on the developing brains of our children. It’s utterly unethical and certainly unscientific to be using these drugs on kids this young.”
Last October, an article in the Herald revealed that the number of children aged 10 to 14 who were taking antidepressants had increased by 280% during the last decade. John Read (right), a professor of clinical psychology, described this figure as “alarming”. He added: “We just have no idea what effect these chemicals have on the developing brains of our children. It’s utterly unethical and certainly unscientific to be using these drugs on kids this young.”
On the other hand, the aforementioned Aileen Blower said that “they can really help young people engage with psychological therapies, get back to school, look after themselves, and definitely reduce suicide risk.”
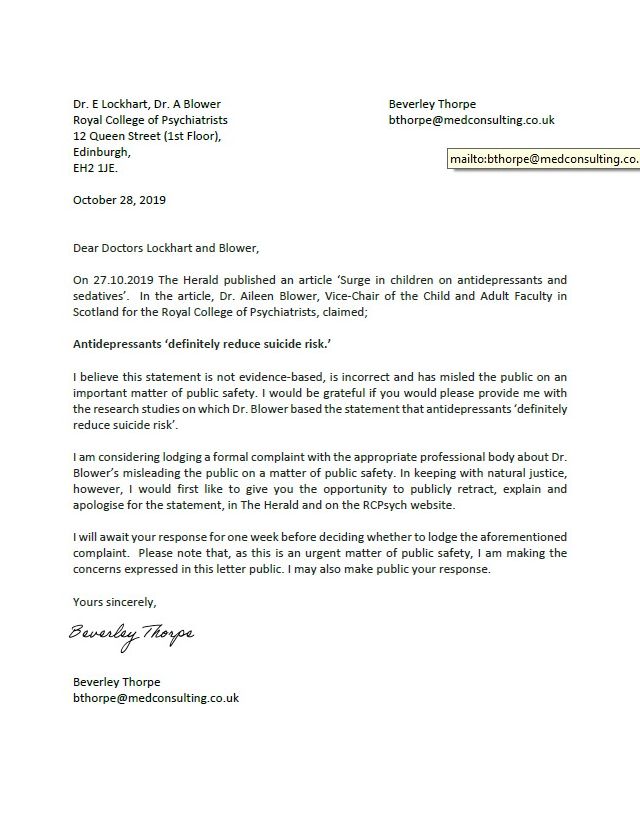 When consultant Beverley Thorpe, who also contributed to the article, read what Dr Blower had said, she wrote (left) to her asking her to retract her statement, which is not only palpably untrue, but reckless.
When consultant Beverley Thorpe, who also contributed to the article, read what Dr Blower had said, she wrote (left) to her asking her to retract her statement, which is not only palpably untrue, but reckless.
SSRI antidepressants are even more likely to induce akathisia in children than in adults. An independent study in New Zealand in 2012 found that 87% of children who had taken their lives had been taking antidepressants at or before the time of their death.
Not only Dr Blower, but her fellow expert witnesses Dr Mockett and Dr Marshall, would have been well aware of the dangers of prescribing antidepressants to children. Yet, shamefully, the three experts chose to remain silent.
Update (October 7th 2020):
At the beginning of this month, Sheriff Lorna Drummond published her report. An article on the BBC website stated that Sophie’s death “might have been prevented with better NHS support”.
The sheriff said that precautions could have included using a structured risk assessment, considering more intensive treatment in the community, involving social work and Sophie’s family, and providing further family therapy to her.
Sophie’s mother Ruth Moss said that her initial reaction was one of relief. She continued: “I have always been of the view that Sophie’s death was preventable and that had Sophie had standard care, she would be alive today. The CAMHS system in Tayside let her and us down.”
The article also provided a link to the Sheriff’s report, which is now in the public domain. The Sheriff began by listing her general findings, one of which was that “Mrs Moss was supplied with insufficient advice regarding prescription of antidepressants for Miss Parkinson”.
In the narrative summary of the events, medication is first mentioned after Sophie was referred to CAMHS. I have transcribed some of the subsequent paragraphs. Direct quotes are in italics; the emphases are my own.
On September 26th 2013, Sophie met with Dr Luke McQuitty, a trainee consultant psychiatrist, for an initial referral discussion. “Her mother attended with her but Miss Parkinson did not want her to go in to the appointment so she waited in the waiting room…He found significant evidence of low mood, anergia, anhedonia (inability to feel pleasure) and biological features of depression. He was keen that she continued follow up with psychological services in the first instance. He prescribed her Fluoxetine 20mg in order that she could maintain her level of function and lift her mood…According to Mrs Moss, the prescription was handed to her in the waiting room where other patients were present. There was no discussion with her about what the medication was for or what the side effects might be. There was no written information except the leaflet inside the box which didn’t mention children.”
In October and November, Ruth met with two of the teachers at Sophie’s school, who “had serious concerns about Miss Parkinson’s mental state. She had been expressing suicidal thoughts to her RE teacher…and threatening to harm herself and run out of school.”
On October 15th, Ruth called a therapist “as she was becoming more and more concerned about Miss Parkinson. Her self-harming had increased and there were cuts from her knees upwards. Her mood continued to be very low.”
On November 6th, Sophie had an initial assessment appointment with two psychologists at CAMHS. “In the notes, it is recorded that Mrs Moss attended for the first five minutes. Mrs Moss doesn’t recall being given any feedback after this appointment. The notes record that Miss Parkinson felt her Fluoxetine prescription had helped lift her mood and felt less need to self-harm over the last few weeks.”
On December 13th, Sophie had an appointment with Dr McQuitty, who “felt there were improvements to make in light of the intense nature of her suicidal thoughts and increased the dose of Fluoxetine to 40mg.”
On January 14th 2014, Ruth telephoned the clinical psychologist to report concerns about Sophie’s moods and self-harm during the school holidays. She asked if Sophie had depression. The psychologist “stated that this may be one of the symptoms, along with anxiety and self-harm, but that the root difficulty with Miss Parkinson appeared to relate to insecurities in her attachments. Mrs Moss was confused by the discussion. Miss Parkinson had been on antidepressant medication for a while, and she couldn’t understand why there seemed to be disagreement over whether or not she was depressed.”
On January 31st, Sophie had an appointment with Dr McQuitty. “The record of this appointment is retrospective, dated 11 March 2014 as the original dictation was misplaced and accidentally destroyed…He described Miss Parkinson as presenting somewhat brighter, had found techniques on reducing self-harm to be useful and had no suicidal ideation at the time of review. He described her compliance with Fluoxetine as patchy and that she has experienced little benefit from it. Although it had initially seemed to produce some improvement in function this had not led to a significant improvement in her mood. He therefore decided to reduce Miss Parkinson’s prescription for Fluoxetine over the next week and she was then to begin a course of Sertraline. Mrs Moss stated that she was handed the prescription in the waiting room, with no discussion about Sertraline’s potential side effects. She wasn’t provided with any information about Sertraline and any increased risks that this might pose.
On February 10th, Ruth had a meeting with Sophie’s therapist, where she expressed deep concerns about Sophie’s suicidal thinking. “She asked what the plan of care for Miss Parkinson was and what her actual diagnosis was, as well as mentioning other mental health disorders. Mrs Moss found [the therapist] to be very vague about Miss Parkinson’s diagnosis suggesting it could be a number of things, including borderline personality disorder. He said that CAMHS used a ‘formulation’ approach instead of giving formal diagnoses. Mrs Moss didn’t have any understanding of this approach and it wasn’t explained to her. She was still unclear of Miss Parkinson’s diagnosis, in spite of her being on antidepressant medication.”
In the early hours of March 1st, Sophie took her life in her bedroom. Toxicology analysis “found only a therapeutic concentration of (antidepressant) Sertraline in the blood of the deceased, all other analyses being negative.”
Sheriff Lorna Drummond’s summary of the inquiry includes a section entitled “Lack of information about prescribed medication”.
The Sheriff writes: “Mrs Moss invited me to find it a relevant fact that Mrs Moss was supplied with insufficient advice regarding the provision of antidepressants prescribed for her daughter. I accept Dr McQuitty’s evidence that he handed Mrs Moss the prescriptions and that he explained to Mrs Moss that Miss Parkinson was being prescribed Fluoxetine and subsequently Sertraline. This is consistent with the records he kept. However I accept Mrs Moss’s evidence that at least so far as the Fluoxetine was concerned, the discussion was fleeting, having taken place in the waiting room and that she was not advised of the rationale for the treatment or the potential side-effects. I also accept her evidence that she was similarly unaware of the rationale behind the Sertraline prescription and was not aware of the side effects nor the need to closely monitor Miss Parkinson at the start of treatment. She was not provided with any written information about either prescribed drug. As explained above it is important to involve parents and carers in the care and treatment of young people so that they can be safely managed. I agree that this was a fact relevant to the circumstances of Miss Parkinson’s death.
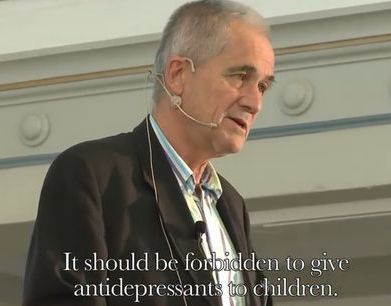
What is missing from this inquiry is any appreciation of the inherent dangers of prescribing antidepressants to children under the age of 18. Back in 2004, NICE Guidelines stated that SSRI antidepressants should not be prescribed to children as the “risk-benefit ratio is poor”. The sole exception was for extreme cases of severe depression, where only Fluoxetine was permitted. Many psychiatrists, such as Professor Peter Gøtzsche (below), believe that, because of the risk of suicidal ideation, no child should ever be prescribed an SSRI antidepressants.
Sheriff Lorna Drummond cannot be expected to be familiar with NICE Guidelines. However, as a prescriber, Dr McQuitty should certainly have known about the dangers of antidepressants. After all, even trainee healthcare assistants are told that “SSRIs have been linked with suicidal thoughts” and that “they might only work for people who are severely depressed.”
And Dr McQuitty should also be familiar with the British National Formulary (BNF), the official handbook from which doctors prescribe. This contains the paragraph: “The use of antidepressants has been linked with suicidal thoughts and behaviour. Where necessary patients should be monitored for suicidal behaviour, self-harm or hostility, particularly at the beginning of treatment or if the dose is changed.” Dr McQuitty changed Sophie’s dosage twice, then changed the brand, putting Sophie at even more risk than she had been during the previous weeks. Yet he chose not to reveal this at the inquiry. More importantly, before Sophie’s death, he kept this information from her mother.
And, of course, the three “experts” – Dr Blower, Dr Mockett and Dr Marshall – would have been well aware of what NICE and the BNF have had to say about the considerable risk of prescribing antidepressants to children. But not one of them had the honesty or decency to reveal that vital evidence to the court.
Related Articles:
The Lost Children (2014, 2015, 2016, 2017, 2018 & 2019)
Why we shouldn’t give Prozac to children
Were these children given Prozac?
Dana’s Human Rights – and ours
Jake, Aged 14 (Part One, Part Two & Part Three)
The Girl from Greater Manchester
Thank you so much Brian for your very important summary of yet another tragic case.
How on earth can this tragic (contrived?) oversight – routinely omitting to investigate and gather, at suicide inquest, such important relevant evidence – go on?
https://fiddaman.blogspot.com/2020/03/uk-national-suicide-prevention-strategy.html